



Diabetes, Medications, and Weight
Should we be concerned that weight loss medication has changed the focus of diabetes care?

Despite what you may have learned, type 2 diabetes is a complex condition, and in 2016, Schwartz et al.1 identified 11 factors that increase blood sugar. Many professionals forget that people with prediabetes typically don't lack insulin; they make too much insulin. This information may not seem important until you connect that the hallmark of type 2 diabetes is insulin resistance.

Imagine insulin as a knife and insulin resistance asks how sharp the knife is. The body compensates for the dullness of the insulin by making more insulin. Over time, the pancreas can't make that amount of insulin, and insulin production declines. The next question becomes, how big is the insulin knife? It is learning to what degree the pancreas can make insulin. The size of a person’s insulin knife declines steadily after diagnosis.

Why is this a problem? Insulin is an anabolic hormone or a hormone that causes weight gain. Many people with type 2 diabetes experience weight gain before being diagnosed. Many researchers wondered if weight gain before the diagnosis could be stopped would it be possible to prevent diabetes. Enter the era of the Diabetes Prevention Project, DPP, which found that lifestyle change can delay the onset of diabetes.
Before 2005, the focus was on eating less (food in general or carbohydrates specifically) to decrease the effects of weight gain with T2D. The problem was that people often gained more weight if their blood sugar was in target. Research in the day reported weight gain, as much as 30 pounds2, was a side effect of having blood sugars in the target range. Another problem was when blood sugar management was intensified; many clients had hypoglycemia. To treat low blood sugar, clients were asked to engage in non-hunger eating, which causes weight gain. Before 1995, most diabetes medications caused low blood sugar and weight gain3.
The Era of Weight Neutral Medication
Metformin was approved in the United States in 1995. It was the first weight-neutral medication available for people with diabetes. With this new hope, diabetes care became preoccupied with weight, specifically not gaining weight to keep the A1C in the target range. In 2001, the Diabetes Prevention Program, DPP reported that 58% of people in the lifestyle arm were able to prevent diabetes. From the website, this is the goal of the DPP, “The DPP looked at whether the DPP Lifestyle Change Program or taking metformin would delay or prevent type 2 diabetes.” yet society read this to mean weight loss, not lifestyle change, produced these results.

Even though Glucagon-like-peptide-1, GLP-1, was discovered in 1980, it wasn't introduced as a medication in 2005. Under the trade name Byetta, this daily injection was the first of its class. GLP-1s are now available in various forms, including oral, daily, and weekly injections. This drug class is the first well-received medication that lowered blood sugar and caused weight loss (Which likely increased in response to prediabetes or low blood sugar).

How GLP1 Works
GLP-1 is a fantastic class of drugs. They work in the gut, muscle, and pancreatitis. They slow digestion, inhibit glucagon secretion, and stimulate insulin with a glucose-dependent mechanism. They also increase the effectiveness of existing insulin and send signals to the brain, increasing the sense of fullness. All of this happens without causing low blood sugar. GLP-1 medication targets many of the 11 systems Dr. Swarts identified as a problem for PWDs. This class of drugs has dramatically changed diabetes care.
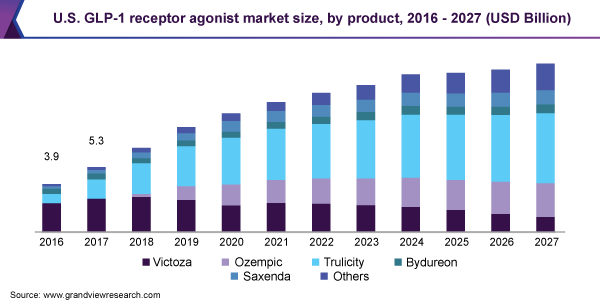
Around 2014, nine years after GLP-1 had been available, there was a change in who these medications were targeted to. With FDA approval for weight loss, GLP-1 was marketed as the magic bullet for higher-weight individuals with diabetes. The image below shows how profitable this class of medication is, and you can read about the marketing of this medication here and here from Ragen Christain. The preoccupation with weight and diabetes has only increased.
In 2017, weight loss surgery for T2D was part of the ADA Standards of Care, SoC.
2023 ADA SoC recommended weight loss of 15%.
The Cost of Diabetes Hasn’t Been Funded
Diabetes is the most expensive chronic illness in the United States4. Consider the additional cost of the GLP-1 class of medication, which is $1300-1700 per month for GLP-1 = $15-20,000 annually.
Is this a good investment? This is an important question because the American Diabetes Association found that 50-60% of all diabetes outcomes are tied to the Social Determinants of Health. Is it a good investment to invest $15,000 annually in a medication when diabetes disproportionately impacts lower-income individuals? What would happen if people with diabetes were provided with this level of support for housing, medical care, and food?
When considering medication, it is essential to factor in the lifetime cost. Is the money spent improving the quality of life? Is the money spent improving the patient's health (outside of weight change)? A new study looked at the impact of GLP-1 on weight for people with diabetes5. This research found the mean weight loss difference between GLP-1 RAs and placebo as an add-on to lifestyle intervention in patients with diabetes was 4% to 6.2% compared to 6.1 to 17.4% in people without diabetes.
You may wonder, would weight loss surgery be less expensive? Weight loss surgery costs $20,000-$25,000 Per the National Institute of Diabetes and Digestive and Kidney Diseases. GLP-1 and Tirzepatide, trade name Mounjaro, medications are often added after weight loss surgery to help prevent weight gain. Why? GLP-1 is said to decrease ‘food noise,’ which can be helpful for people who ‘always feel hungry.’ The question becomes, what is causing this chronic hunger? Is it just diabetes, or could it be a coping mechanism related to chronic dieting, trauma, food insecurity, or diabetes?
GLP-1 medication has side effects that include pancreatitis, nausea, and decreased nutrient intake, which can increase malnutrition, a concern for people over 65, who often experience a change in taste and appetite. Combined with a person’s age, cost, and side effects, these medications can trigger disordered eating patterns, specifically, meal skipping, low protein intake, inadequate fiber, vitamins, and minerals, and lack of interest in eating/social isolation.

Returning to the knife analogy, how much work are we asking a smaller, duller knife to do? This is when food quality is helpful, specifically the Food As Medicine movement. It is a complex issue because diabetes is a chronic condition that changes as it progresses. Additionally, it is a condition that impacts individuals as they age, and this also intersects with other factors, including a decline in overall health and income and an increase in isolation.
Should weight loss be the primary goal in diabetes care?
How do the efforts to promote weight loss via surgery or medication connect to our current efforts to address the social determinants of health by providing medically tailored meals and increasing food access? How does quality of life factor into diabetes care? How are GLP-1s part of our efforts to decrease food insecurity? Are efforts to address the SDOH adequately funded compared to paying for WLS and GLP-1 medication? Is weight stigma behind the push for GLP1?
In Summary
Type 2 diabetes is a complex condition with various factors affecting blood sugar, including insulin resistance that triggers the overproduction of insulin.
Weight gain is a common issue for people with type 2 diabetes, and before 2005, the focus of care was on reducing food intake or carbohydrates to control weight.
Metformin, introduced in 1995, was the first weight-neutral medication for diabetes, shifting the focus towards preventing weight gain.
The introduction of GLP-1 medications in 2005 marked a significant change in diabetes care, as they didn't cause weight gain and addressed multiple factors affecting diabetes.
The cost of diabetes care, particularly GLP-1 medications and weight loss surgery, is a concern, considering their high expenses and potential impact on long-term health and quality of life.
Schwartz, S. S., Epstein, S., Corkey, B. E., Grant, F. A., & Aguilar, R. B. (2016). The Time Is Right for a New Classification System for Diabetes: Rationale and Implications of the β-Cell–Centric Classification Schema. Diabetes Care, 39(2), 179-186. https://doi.org/10.2337/dc15-1585
Franz, M. J., et al. (2015). Lifestyle Weight-Loss Intervention Outcomes in Overweight and Obese Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Journal of the Academy of Nutrition and Dietetics, 115(9), 1447-1463
Acarbose was invented in 1970. It is a starch-blocker. It was not well received in the US and was not included in this discussion.
Centers for Disease Control and Prevention. (2022, December 21). Health and economic benefits of diabetes interventions. Centers for Disease Control and Prevention. https://www.cdc.gov/chronicdisease/programs-impact/pop/diabetes.htm#:~:text=Diabetes%20is%20the%20most%20expensive%20chronic%20condition%20in%20our%20nation.&text=%241%20out%20of%20every%20%244,caring%20for%20people%20with%20diabetes.&text=%24237%20billion%E2%80%A1(a)%20is,(a)%20on%20reduced%20productivity.
Jensterle, M., Rizzo, M., Haluzík, M., & Janež, A. (2022). Efficacy of GLP-1 RA Approved for Weight Management in Patients With or Without Diabetes: A Narrative Review. Advances in Therapy, 39(6), 2452-2467. https://doi.org/10.1007/s12325-022-02153-x